What Recent Resarch Says About Liposomal Iron in IBD
Iron is one of the most fundamental minerals in the human body. Every red blood cell needs it. Every oxygen molecule transported in your blood depends on it. And yet, for millions of people living with Inflammatory Bowel Disease, getting enough iron into their system is a problem that neither diet nor conventional supplements can reliably solve.
The reason is not complicated, but it is often misunderstood.
The gut wall — already inflamed, already compromised — turns out to be a remarkably effective barrier against the very iron that patients need most. Standard oral iron salts make this barrier more hostile. And so, quietly but consistently, a large proportion of IBD patients remain anaemic despite being on iron therapy.
Liposomal iron does not just offer a gentler alternative. It changes the underlying delivery mechanism entirely. This blog explains what that means in practice — for patients, for clinicians, and for the manufacturers and CDMOs building the next generation of IBD-focused iron formulations.
Key Takeaways:
- Conventional oral iron is biologically incompatible with the IBD gut: It is not just poorly tolerated — ferrous salts actively worsen mucosal inflammation, disrupt the gut microbiome, and are blocked by the elevated hepcidin that IBD itself produces. The failure is mechanistic, not incidental.
- Liposomal iron solves the problem at the point of delivery: By encapsulating ferric pyrophosphate within a phospholipid bilayer and delivering it intracellularly via endocytosis, liposomal iron bypasses the hostile gut lumen, avoids free radical generation, and achieves meaningful absorption even in inflamed intestinal tissue.
- For manufacturers, getting the API right is the whole game: Liposomal iron formulation quality is determined upstream — by encapsulation efficiency, particle size, phospholipid purity, and oxidative stability. Sourcing from a GMP-certified partner like WBCIL, with full batch documentation and proven technical capability, is not optional. It is the foundation of a product that can be trusted.

Iron Deficiency Anaemia in IBD: Bigger Than Most People Realise
Iron deficiency anaemia (IDA) is the most common systemic complication of Inflammatory Bowel Disease. Studies estimate it affects between 36% and 76% of IBD patients depending on disease activity and clinical setting [1]. In hospitalised patients, that number climbs higher still.
What makes IDA in IBD particularly difficult to treat is that it does not have a single cause. It is usually the result of several overlapping mechanisms happening at the same time:
Chronic Intestinal Blood Loss
Active inflammation erodes the gut mucosa. Ulcerated tissue bleeds — sometimes visibly, often microscopically. This steady loss of blood means a steady loss of iron-laden red blood cells. Even when the patient is eating iron-rich food and taking supplements, the loss can outpace replenishment.
Impaired Mucosal Absorption
Iron absorption from food takes place primarily in the duodenum and upper jejunum. In IBD, these sections of the small intestine are frequently inflamed. The enterocytes responsible for transporting iron across the gut wall are damaged and functionally impaired — they simply cannot do their job at full capacity.
Hepcidin-Mediated Iron Restriction
This is the piece that is least understood outside specialist circles, but it matters enormously. Hepcidin is a liver-derived peptide hormone that acts as the master regulator of iron metabolism. When inflammation is active — as it is in IBD — the body produces elevated levels of hepcidin [2].
High hepcidin does two things. First, it triggers the internalisation and degradation of ferroportin, the only known cellular iron exporter. This traps iron inside enterocytes and macrophages, preventing it from entering the bloodstream. Second, it reduces the expression of duodenal iron transporters, further suppressing absorption.
In short: even if iron reaches the gut, hepcidin actively blocks it from entering circulation. This is not a side effect of IBD — it is a direct biological consequence of systemic inflammation.
Dietary Restriction
Many IBD patients follow restricted diets to manage their symptoms, often limiting red meat, legumes, and fortified cereals — all significant dietary iron sources. This compounds the absorption problem further.
Why Conventional Oral Iron Makes Things Worse, Not Better
Conventional oral iron — in the form of ferrous sulphate, ferrous fumarate, or ferrous gluconate — has been the standard first-line treatment for IDA for decades. It is cheap, widely available, and well understood. It is also a poor fit for the IBD gut, for reasons that go beyond tolerability.
Free Radical Generation in the Gut Lumen
When ferrous iron (Fe²⁺) salts dissolve in the intestine, they release free ionic iron directly into the gut lumen. This ionic iron is highly reactive. It participates in the Fenton reaction — a chemical process that generates hydroxyl radicals, one of the most damaging reactive oxygen species known [3].
In a healthy gut, the mucosal lining has enough antioxidant capacity to handle modest amounts of this oxidative stress. In an already-inflamed IBD gut, it does not. The result is measurable worsening of mucosal oxidative damage — the exact opposite of what a patient with active intestinal inflammation needs.
Microbiome Disruption
Only a fraction of orally administered iron is absorbed in the small intestine. The rest continues into the colon, where it becomes a nutrient substrate for iron-dependent pathogenic bacteria — including strains of Escherichia coli and Clostridium — that are already overrepresented in the IBD microbiome [3].
This selective feeding of pathogenic species worsens the microbial dysbiosis that characterises IBD and has been shown to correlate with increased disease activity. Giving conventional oral iron to an IBD patient is, in microbiome terms, adding fuel to a fire.
Low Actual Bioavailability
Given the combination of mucosal damage, hepcidin elevation, and poor tolerability leading to skipped doses, the actual bioavailability of conventional oral iron in active IBD is often estimated at 5–10% [1]. Patients who do tolerate the side effects may still not be getting meaningful therapeutic benefit.
It is this combination — mucosal harm, microbiome disruption, and poor absorption — that has pushed clinicians toward intravenous iron for moderate-to-severe IBD-related IDA. But IV iron requires clinical infrastructure and carries its own risks. There is a genuine clinical gap that oral liposomal iron is well positioned to fill.
The Liposomal Iron Delivery System: Mechanism Explained
Understanding why liposomal iron works requires a brief look at what a liposome actually is and how it interacts with the gut.
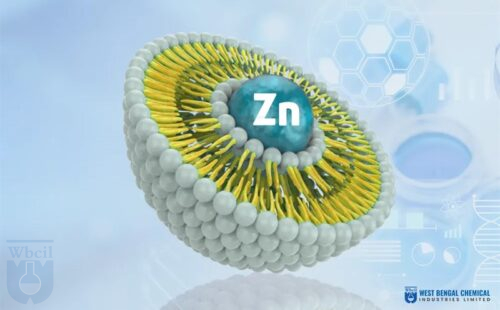
A liposome is a spherical vesicle made of a phospholipid bilayer — the same basic structure as a cell membrane. Its core can be loaded with water-soluble compounds (like iron salts), and its outer shell is hydrophobic, meaning it does not dissolve in water. This physical structure is what makes liposomal delivery fundamentally different from dissolving an iron tablet.
Liposomal Iron Absorption Mechanism in Inflammatory Bowel Disease
When a liposomal iron formulation is ingested, the encapsulated iron travels through the stomach and into the small intestine without being released into the gut lumen. The phospholipid shell protects the iron payload from the acidic gastric environment and prevents premature dissolution.
At the level of the intestinal epithelium, the liposome interacts directly with the enterocyte membrane. Because both structures share the same phospholipid bilayer architecture, the liposome fuses with the cell membrane and delivers its iron content intracellularly via endocytosis [4]. The iron enters the enterocyte directly — without ever being exposed as free ionic iron in the gut lumen.
From inside the enterocyte, iron is then processed normally and exported into the bloodstream via ferroportin — the same transporter that hepcidin targets. This is an important nuance: liposomal iron does not completely bypass hepcidin. In states of very high hepcidin (severe active inflammation), even liposomal iron absorption will be partially restricted. However, because the iron reaches ferroportin already inside the cell — rather than competing for uptake at the luminal surface — the efficiency of absorption is significantly higher than with conventional iron salts [4].
The key insight: liposomal iron does not fight the inflamed gut environment. It sidesteps it. Iron is delivered into the cell before the gut’s hostile chemistry can interfere.
Why Ferric Pyrophosphate Is the Preferred Iron Form
Most pharmaceutical-grade liposomal iron products use ferric pyrophosphate (Fe₄(P₂O₇)₃) as the encapsulated iron compound. There are specific reasons for this choice:
- Ferric pyrophosphate is a stable, insoluble iron salt that does not dissociate in water at physiological pH — making it ideal for liposomal encapsulation without risk of early release.
- It has a well-established safety profile with minimal pro-oxidant activity compared to ferrous salts
- Its molecular size and charge characteristics are compatible with efficient phospholipid bilayer encapsulation
- Clinical evidence supports its efficacy when delivered via liposomal technology, with documented haemoglobin restoration in IDA patients [4] [5]

Head-to-Head: Liposomal Iron vs Conventional Oral Iron in IBD
What the Clinical Evidence Shows
The body of clinical evidence supporting liposomal iron in IBD and related inflammatory conditions is now substantial enough to influence prescribing practice in several markets.
A multicentre randomised controlled trial demonstrated that liposomal iron produced haemoglobin increases comparable to intravenous iron in IBD patients, with a markedly superior gastrointestinal tolerability profile and no increase in disease activity [4].
Studies comparing liposomal ferric pyrophosphate to ferrous sulphate in patients with inflammatory gut conditions consistently show three to four times higher fractional iron absorption with the liposomal form [5].
Patient-reported outcome data shows significantly lower rates of GI adverse events — nausea, bloating, stool changes — with liposomal iron versus conventional oral iron, translating into better real-world adherence.
Faecal calprotectin levels — a marker of intestinal inflammation — do not rise following liposomal iron administration, unlike with ferrous sulphate, supporting its safety in active IBD [4].
It is important to be clear about what liposomal iron is not: it is not a replacement for intravenous iron in severe, rapidly progressing IDA or in patients with very high disease activity. What it offers is a clinically meaningful oral option for mild-to-moderate iron deficiency maintenance, post-IV top-up therapy, and patients who are intolerant of or unable to access IV iron.
The Manufacturing Opportunity: What CDMOs and Generic Manufacturers Need to Know
The clinical case for liposomal iron is solid. The commercial case is becoming equally compelling.
Global IBD prevalence has been rising steadily for three decades. An estimated 10 million people worldwide now live with the condition [1], and IDA affects a significant proportion of them chronically — meaning ongoing iron supplementation is a permanent fixture of their management. This is not a one-time treatment market. It is a maintenance market.
Advantages of Liposomal Iron for Generic Pharma Manufacturers
- Differentiated positioning — liposomal iron cannot be dismissed as a commodity product. Its mechanism, tolerability data, and clinical evidence create genuine product differentiation.
- Premium market placement — manufacturers command meaningfully higher price points than standard iron salts, with consumers and clinicians willing to pay for demonstrated tolerability.
- Expanding clinical indications — beyond IBD, liposomal iron has growing evidence in pregnancy-related IDA, chronic kidney disease, post-bariatric surgery, and restless legs syndrome, broadening total addressable market.
- Regulatory pathway clarity — in most markets, liposomal iron qualifies as a food supplement or nutraceutical rather than a pharmaceutical drug, reducing regulatory time and cost.
Formulation Complexity: What Manufacturers Must Get Right
Liposomal iron is not technically simple to manufacture. The encapsulation process introduces variables that standard iron salt formulations do not have to manage:
- Particle size distribution — Optimal absorption requires vesicles in the 100–200 nm range. Particles outside this range show significantly reduced endocytotic uptake efficiency
- Iron encapsulation efficiency — The proportion of iron successfully enclosed within the liposome — rather than remaining in the aqueous phase — directly affects product potency and must be validated per batch
- Oxidative stability — Ferric iron and unsaturated phospholipids can interact over time. Formulation antioxidants and inert gas packaging are typically required
- pH and ionic strength — The aqueous core environment affects iron solubility and bilayer integrity throughout shelf life
These variables mean that the starting material — the liposomal iron API itself — determines much of the product quality ceiling. A CDMO cannot compensate in processing for substandard raw material. This makes supplier selection genuinely consequential.
B2B Sourcing for Liposomal Iron Ferric Pyrophosphate: Key Criteria
When evaluating suppliers for pharmaceutical-grade liposomal iron, these are the parameters that distinguish reliable manufacturing partners from commodity distributors:
- GMP certification with full batch documentation and traceability
- Verified encapsulation efficiency per batch, not just iron content
- Documented particle size data (DLS measurement) with specification ranges
- Phospholipid purity data with defined fatty acid profiles
- Stability data under accelerated and real-time storage conditions
- Regulatory dossier support — CoA, MSDS, TSE/BSE declarations, allergen statements
- Consistent supply capability with minimum lead time variability
WBCIL (West Bengal Chemical Industries Limited) manufactures patented pharmaceutical-grade liposomal iron — including liposomal ferric pyrophosphate — for CDMOs, generic manufacturers, and nutraceutical brands globally. Built on GMP-certified infrastructure with deep expertise in liposomal technology, WBCIL supplies both the finished liposomal ingredient and technical documentation required for downstream product development and regulatory submissions.
- Stein, J., et al. (2021). Management of iron deficiency anaemia in inflammatory bowel disease — a practical approach. Annals of Gastroenterology, 34(2), 134–148.
- Ganz, T. (2019). Anemia of Inflammation. New England Journal of Medicine, 381(12), 1148–1157.
- Kortman, G.A.M., et al. (2014). Oral iron supplementation: potential implications for the gut microbiome and metabolome. FEMS Microbiology Ecology, 87(2), 445–454.
- Pisani, A., et al. (2015). Liposomal iron versus intravenous iron in patients with IBD: a multicentre, open-label, randomised, controlled trial. The Lancet Haematology, 2(11), e471–e478.
- Wegmüller, R., et al. (2014). Bioavailability of microencapsulated ferric pyrophosphate in adults with low iron stores. Journal of Food Science, 79(5), N991–N1000.
Liposomal iron encapsulates ferric pyrophosphate inside a phospholipid bilayer (liposome). Unlike conventional ferrous salts, it does not dissolve freely in the gut lumen. Instead, it fuses with intestinal cell membranes and delivers iron intracellularly via endocytosis — a process that avoids free radical generation and mucosal irritation entirely.
Three overlapping mechanisms: (1) inflamed enterocytes cannot transport iron efficiently across the gut wall; (2) elevated hepcidin — produced in response to systemic inflammation — degrades ferroportin and blocks iron export into the bloodstream; and (3) conventional iron salts worsen local inflammation, making all of the above worse.
Not completely. Hepcidin acts on ferroportin, which is used by enterocytes to export iron into circulation — and liposomal iron still depends on this pathway. However, because liposomal iron is delivered inside the enterocyte rather than competing for uptake at the luminal surface, it is less affected by luminal hepcidin activity and achieves higher net absorption in inflamed tissue.
Ferric pyrophosphate (Fe₄(P₂O₇)₃) is the standard choice. It is stable, insoluble at physiological pH, does not dissociate prematurely in the gut, and has low pro-oxidant activity compared to ferrous salts — all of which make it technically well-suited to liposomal encapsulation.
Clinical evidence suggests liposomal iron does not worsen mucosal inflammation or raise faecal calprotectin levels — a key distinction from conventional oral iron, which can trigger flares. That said, in severe active IBD with very high inflammatory burden, IV iron remains the preferred route for rapid correction.
WBCIL (West Bengal Chemical Industries Limited) is a WHO GMP-certified supplier of liposomal iron for CDMOs and generic manufacturers globally. They provide full batch documentation, particle size data, encapsulation efficiency reports, and regulatory support. Visit www.wbcil.com for technical information and sample requests.
Key parameters are encapsulation efficiency (%), mean particle size (nm) by DLS, phospholipid purity and fatty acid profile, iron content per unit, oxidative stability data, pH of aqueous phase, and GMP certification with full CoA and traceability documentation