Why Liposomal Calcium Absorbs Differently: The Science of Endocytosis, Paracellular Transport, and Bypassing TRPV6
In the evolving field of bone health, liposomal calcium stands as a revolutionary departure from the inefficient, high-dose mineral supplements of the past. While calcium is vital for skeletal integrity, its bioavailability has historically been strangled by the rigid physiological bottlenecks of the human gut. However, targeted delivery of encapsulated ions to the intestinal brush border has significantly increased liposomal calcium absorption.
This approach offers a robust mechanistic solution to the pharmacokinetic bottlenecks of traditional mineral therapy, ensuring higher flux across the epithelium via multiple simultaneous transport routes-endocytosis, paracellular transport, and lymphatic uptake, finally providing a mechanistic solution to the delivery failures that have long plagued conventional mineral therapy.
Key Takeaways
- Bypassing TRPV6: Liposomal calcium uses endocytosis to bypass saturable, Vitamin D-dependent transport channels.
- Vascular Safety: Slow-release kinetics prevent hypercalcemic spikes and arterial mineral deposition.
- Shielded Bioavailability: Encapsulation protect calcium from inhibitory phytates and oxalates.

How Conventional Calcium Is Absorbed – and Where It Falls Short
The physiological constraints of traditional calcium delivery systems are centred on a rigid, saturable transport architecture. Understanding the difference between liposomal calcium and traditional calcium salts requires a breakdown of this transcellular bottleneck:
- TRPV6 Entry: Luminal calcium ions must enter enterocytes through the transient receptor potential vanilloid type 6 (TRPV6) channel. This serves as the primary, rate-limited gatekeeper for mineral influx.
- Intracellular Shuttling: Once internalised, ions are bound and transported by the protein calbindin-D9k [1]. This step is strictly Vitamin D-dependent, meaning mineral uptake is tethered to the patient’s hormonal status.
- Basolateral Export: The final step involves exporting ions into the bloodstream via the PMCA1b pump [2].
Saturation and Hypercalcemia: Because this three-step pathway is easily saturated, high doses of calcium salts overwhelm the system. This results in transient post-prandial hypercalcemia- a 10–15% serum spike associated with increased cardiovascular risk [3]. - The Liposomal Advantage: Bypassing this bottleneck is critical for both therapeutic efficacy and long-term safety, as it prevents the systemic stress caused by the rapid influx of free ions into the vascular compartment.
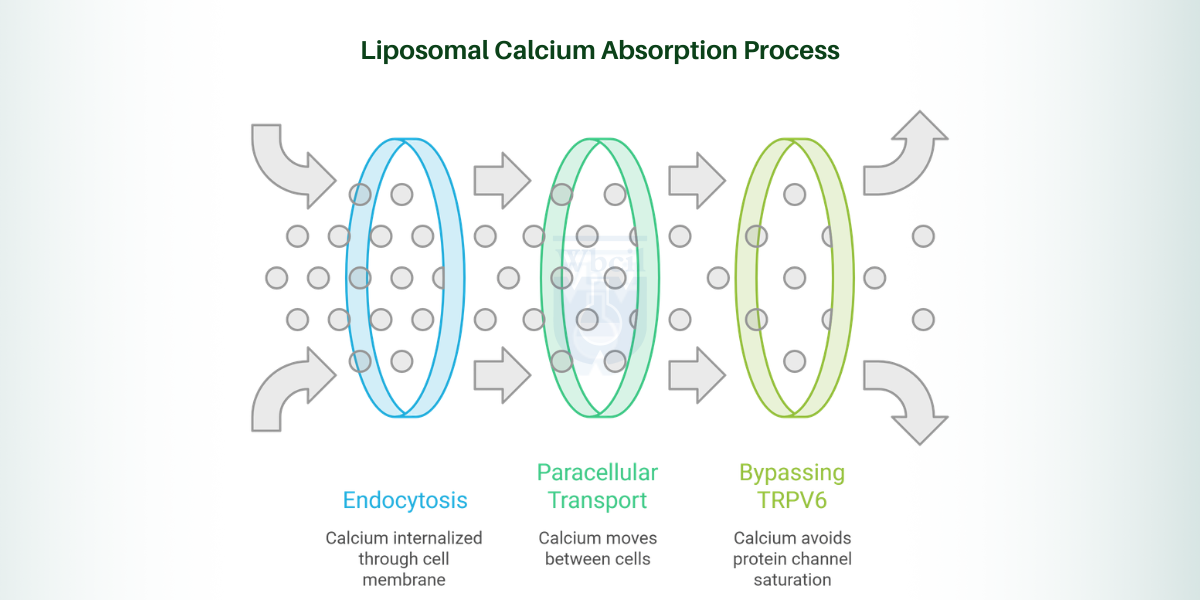
The Three Absorption Pathways That Make Liposomal Calcium Work Differently
The efficacy of liposomal calcium absorption stems from its ability to engage multiple uptake routes simultaneously. Liposomal calcium utilises intestinal calcium delivery systems that operate independently of traditional regulatory constraints.
Pathway 1: Endocytosis — The Cellular “Swallowing” Mechanism
The calcium endocytosis mechanism is the most significant departure from traditional mineral transport. Liposomes consist of phospholipid bilayers that structurally mimic cellular membranes and can trigger endocytosis [4]. In this process, the entire liposomal calcium is internalised without crossing the apical membrane through ion channels.
This calcium endocytosis mechanism completely circumvents the reliance on TRPV6 and calbindin-D9k. Consequently, liposomal calcium absorption becomes non-linear and far less dependent on the patient’s Vitamin D status. This pathway remains active even in ageing populations where active Vitamin D-dependent transport naturally declines.
By leveraging the mechanism, the body maintains mineral homeostasis even when traditional pathways are compromised.
Pathway 2: Paracellular Transport – Moving Between the Cells
Paracellular calcium absorption refers to the passive movement of calcium through tight junctions between enterocytes, driven by an electrochemical gradient. While traditional calcium salts cause a rapid spike and rapid clearance, liposomal formulations maintain a sustained luminal calcium concentration gradient.
Furthermore, the phospholipid shell protects the mineral core from binding to dietary inhibitors such as phytates and oxalates in the lumen. In traditional supplements, these inhibitors precipitate calcium, rendering it unabsorbable. The bioavailability of liposomal minerals is preserved because the calcium remains shielded, maintaining the available ion pool for paracellular calcium absorption.
Pathway 3: Bypassing TRPV6-Why Rate-Limiting Transporters No Longer Apply
The most significant constraint on mineral uptake is the saturation of protein channels. Bypassing TRPV6 calcium transport is the primary reason for the significant enhancement in liposomal calcium absorption, resulting in higher bioavailability at lower relative doses. Once the TRPV6 channels are occupied, additional oral calcium passes through unabsorbed.
By bypassing TRPV6 calcium transport, liposomal delivery sidesteps this metabolic ceiling. The result is a prolonged elevation in serum calcium that avoids the dangerous hypercalcemic spike while delivering superior mineral bioavailability. Current pharmacokinetic data indicate that bypassing the TRPV6 transporter enables a steady-state mineral concentration that more closely resembles natural dietary intake. This unique profile of intestinal calcium delivery is why liposomal Calcium absorption is increasingly favoured in clinical settings.
The Calcium Paradox: Why Better Absorption Alone Is Not Enough
The “calcium paradox” refers to the state in which skeletal mineral deficiency coexists with ectopic vascular calcification. The mechanisms of liposomal calcium cardiovascular support are fundamentally rooted in controlled-release kinetics, which prevent the systemic volatility seen with traditional delivery. Unlike conventional supplements that trigger transient hypercalcemia and overwhelm inhibitory proteins such as Matrix Gla Protein (MGP), controlled liposomal calcium absorption maintains mineral levels within a physiological range.
This unique advantage of novel liposomal calcium nutraceutical systems for bone health ensures the mineral is directed into the bone matrix rather than being deposited in the arterial tunica media, thereby mitigating the risk of ectopic vascular calcification.
The Lymphatic Absorption Route: How Liposomal Calcium Enters the Body Like Dietary Fat
A distinct advantage of liposomal delivery systems is the engagement of the lymphatic system [5]. Due to their lipid bilayer structure, liposomal calcium is absorbed via the intestinal lymphatic pathway, thereby enabling a significant fraction of the mineral load to bypass immediate hepatic first-pass metabolism.
Instead of entering the portal vein, the vesicles are integrated into chylomicrons and transported through the intestinal lymphatic system. This allows the mineral to enter systemic circulation gradually via the thoracic duct, contributing to the “slow-release” profile that defines the bioavailability of liposomal minerals.
This lymphatic route contributes to the slower, more sustained serum concentration profile that characterises liposomal calcium absorption.
The Lymphatic Absorption Route: How Liposomal Calcium Enters the Body Like Dietary Fat
A distinct advantage of liposomal delivery systems is the engagement of the lymphatic system [6]. Due to their lipid bilayer structure, liposomal calcium is absorbed via the intestinal lymphatic pathway, thereby enabling a significant fraction of the mineral load to bypass immediate hepatic first-pass metabolism.
Instead of entering the portal vein, the vesicles are integrated into chylomicrons and transported through the intestinal lymphatic system. This allows the mineral to enter systemic circulation gradually via the thoracic duct, contributing to the “slow-release” profile that defines the bioavailability of liposomal minerals.
This lymphatic route contributes to the slower, more sustained serum concentration profile that characterises liposomal calcium absorption.
Formulation Science Behind the Absorption Advantage
The bioavailability of liposomal minerals is a function of rigorous formulation engineering. WBCIL’s LipoedgeTM liposomal calcium utilises specific parameters to ensure stability:
- Particle Size (<300 nm): Optimises both the calcium endocytosis mechanism and colloidal stability. WBCIL’s Liposomal Calcium features a validated particle size of 200-300 nm.
- Zeta Potential (< −30 mV): High-quality formulations ensure vesicles remain intact. WBCIL’s formulation is validated at −30.67 mV.
- Encapsulation Efficiency: WBCIL’s liposomal calcium achieves a >70% encapsulation efficiency benchmark, protecting the mineral from inhibitors.
Who Benefits Most?
The mechanistic advantages of liposomal calcium absorption are most relevant for:
- Ageing Adults (Vitamin D and Transporter Deficiency): With declining TRPV6 expression, the calcium endocytic pathway provides a critical bypass.
- Postmenopausal Women (Cardiovascular and Skeletal Risk): Benefits from the controlled-release kinetics inherent in liposomal calcium absorption.
- Individuals with Gastrointestinal Conditions (IBS, IBD, Celiac benefitt most from paracellular calcium absorption, as the liposomal structure protects the mineral core from luminal irritants and dietary inhibitors
- Patients on Proton-Pump Inhibitors (PPIs): Liposomal calcium absorption works independently of the gastric acid required for traditional salts
How Does WBCIL’s Liposomal Calcium Deliver Where Conventional Supplements Cannot?
WBCIL’s LipoedgeTM technology has engineered a definitive solution to the “absorption ceiling” that limits the effectiveness of traditional mineral therapy.
- Bypassing the Transcellular Bottleneck: Conventional calcium relies almost exclusively on the TRPV6 transcellular pathway. This acts as a physiological bottleneck; once these channels are occupied, net absorption plateaus regardless of dose.
- Simultaneous Multi-Pathway Engagement: WBCIL’s liposomal calcium circumvents this limitation by concurrently engaging both the calcium endocytic pathway and paracellular calcium absorption.
- Enhanced Net Bioavailability: This diversified entry strategy ensures a significantly higher net bioavailability of liposomal minerals, ensuring the payload is internalised even at higher concentrations.
- Mitigation of Adverse Effects: By utilising these advanced intestinal calcium delivery systems, WBCIL ensures efficient internalisation, eliminating the gastrointestinal distress and poor compliance typically caused by the accumulation of unabsorbed calcium salts in the intestinal lumen.
Conclusion: Absorption Is Not Just About the Dose – It Is About the Pathway
The clinical superiority of liposomal calcium absorption is defined by its ability to engage a tri-modal uptake strategy, encompassing calcium endocytosis, paracellular absorption, and lymphatic absorption. By bypassing TRPV6-mediated calcium transport, these formulations provide a dual therapeutic benefit: optimised skeletal mineral deposition and enhanced cardiovascular safety by preventing hypercalcemic spikes.
The science behind this shift is not merely theoretical; it is quantifiable through precise pharmacokinetic profiles and validated engineering parameters. WBCIL’s liposomal calcium exemplifies this rigorous approach to achieve targeted delivery. This novel liposomal calcium nutraceutical system for bone health ensures that mineral delivery is no longer limited by intestinal saturation but is instead governed by advanced cellular uptake. Ultimately, the bioavailability of liposomal minerals produced by WBCIL’s LipoedgeTM Technology ensures that calcium is effectively partitioned into target tissues, marking a significant advancement in precision mineral supplementation.

- Schröder, B., Schlumbohm, C., Kaune, R., & Breves, G. (1996). Role of calbindin-D9k in buffering cytosolic free Ca2+ ions in pig duodenal enterocytes. The Journal of physiology, 492 ( Pt 3)(Pt 3), 715–722.
- Krebs J. (2022). Structure, Function and Regulation of the Plasma Membrane Calcium Pump in Health and Disease. International journal of molecular sciences, 23(3), 1027.
- Reid, I. R., Birstow, S. M., & Bolland, M. J. (2017). Calcium and Cardiovascular Disease.Endocrinology and metabolism (Seoul, Korea), 32(3), 339–349.
- Straubinger, R. M., Hong, K., Friend, D. S., & Papahadjopoulos, D. (1983). Endocytosis of liposomes and intracellular fate of encapsulated molecules: encounter with a low pH compartment after internalization in coated vesicles. Cell, 32(4), 1069–1079.
- Ahn, H., & Park, J. H. (2016). Liposomal delivery systems for intestinal lymphatic drug transport.Biomaterials research, 20, 36.
Liposomal calcium exploits endocytosis, paracellular transport, and lymphatic routes to bypass the easily saturated, Vitamin D-dependent transporters used by regular supplements. This multi-pathway approach increases bioavailability while preventing the dangerous serum spikes linked to cardiovascular risk.
TRPV6 is a rate-limiting protein channel that acts as a bottleneck for conventional calcium absorption, especially as its efficiency declines with age. Liposomal systems bypass this gateway via endocytosis, ensuring consistent mineral uptake regardless of transporter availability or Vitamin D status.
No; its controlled-release kinetics prevent the sharp 10–15% serum spikes that overwhelm the system and lead to arterial calcification. Maintaining a physiological level prevents the “calcium paradox” and protects vascular health.
Vesicles engineered between 200–300 nm provide the optimal balance of structural stability and endocytic uptake. Sizes outside this window either risk fragility or significantly reduced absorption efficiency during intestinal transit.
Yes, because it utilises endocytosis and paracellular pathways that function independently of the Vitamin D-regulated TRPV6 channel. This makes it a superior option for aging adults or those with deficiencies who cannot efficiently absorb traditional calcium salts.
Liposomal technology encapsulates ions within a phospholipid bilayer that mimics cell membranes, enabling direct cellular uptake and protection against dietary inhibitors. This structural advantage ensures the mineral remains available for absorption throughout the entire length of the small intestine.
Unlike traditional calcium salts that rely on transporters and vitamin D, liposomal calcium utilises multiple non-saturable entry routes simultaneously. When the primary transport channels are full, the endocytic and paracellular pathways remain open to maintain steady mineral influx.